
training resources
Speech and Language Pathologists in the Public Schools
by Fran Kakuska & Kathy Battles (1980's)



Children with physical disabilities often have accompanying speech and/or language disorders. These deficits can be extremely varied – ranging from a mild slurring of speech and/or minor grammatical errors to a totally non-verbal state requiring an augmentative communication system. The speech/language pathologist is the person responsible for the evaluation and treatment of these deficits.
EDUCATIONAL AND CERTIFICATION REQUIREMENTS
The American Speech, Language, and Hearing Association (ASHA, 1985) defines a speech/language pathologist as an individual with an academic degree and/or certification in speech and language pathology (or communication disorders) who is qualified to diagnose speech, language, and voice disorders and to prescribe and implement therapeutic measures. The official title, as determined by ASHA, is Speech and Language Pathologist. On a practical level, the term speech and language therapist or speech and language clinician appears to be a somewhat more appropriate label in a school setting, while someone in a medical environment would generally use the title, speech and language pathologist. Speech and language pathologists are employed in a variety of settings which include schools, hospitals, clinics, universities and research centers, and private practice. Regardless of the setting, however, the speech pathologist's role, responsibilities, and competencies should meet the specific needs of the clientele being served. Educational requirements for becoming a speech/language pathologist include a master's degree with a major emphasis on speech/language pathology with a broad general education background in areas such as human psychology, the physical sciences, human anatomy and physiology, and educational coursework. The individual must also have a minimum of 300 clock hours of supervised clinical experience with individuals who present a variety of communication disorders (ASHA Handbook, 1984). After graduation, many speech and language pathologists pursue requirements for obtaining a Certificate of Clinical Competence which is issued by ASHA. This involves passing the National Examination in Speech, Language Pathology and Audiology and fulfilling a Clinical Fellowship Year (CFY) of full-time professional experience which requires supervision by a certified speech and language pathologist (ASHA, 1984). This CFY supervising pathologist evaluates the Clinical Fellow based on at least 36 supervisory activities and submits a report to ASHA at the end of the CFY year documenting the number of observations and meetings and describing the overall competencies of the candidate. (ASHA, 1984) The candidate's records are then reviewed and the Certificate of Clinical Competence is awarded if all the requirements have been met and the proper fees are paid. Once awarded the CCC, the certificate holder is required to adhere to ASHA's code of ethics which stresses the professional responsibilities of speech/language pathologists in providing services. (ASHA, 1986) (Appendix A) Although all of the principles are important, the focus is placed on providing services that uphold the welfare of the person being served. If a speech/language pathologist does not feel qualified to treat a specific disorder, he/she should refer to another professional who has expertise in that area or assume the responsibility for continuing his/her
education to increase his/her clinical competence. (ASHA, 1982) Certification is maintained by paying an annual fee. Although not required, members are encouraged to seek continuing education to update knowledge regarding the advances that are being made in the profession. Individuals may seek an Award for Continuing Education (ACE) which involves:
accruing seven CEU's (six of which are to be received from sponsors approved by the Continuing Board of ASHA, or
completing six semester hours of academic coursework from an approved sponsor, or
accruing a combination of each of these, or
retaking the national exam.
The ACE is valid for three years during which time the requirements may be completed for renewal. (ASHA, May 1984)
COMMUNICATION DISORDERS DEFINED
ASHA defines a communication disorder as an impairment in the ability to: 1) receive and/or process a symbol system; 2) represent concepts or symbol systems; 3) transmit and use symbol systems. A speech disorder is defined as an impairment of voice, articulation, and/or fluency as they are observed in the transmission and use of speech. A language disorder is defined as an impairment or deviant development of comprehension and/or use of a spoken or written symbol system. The language disorder may involve: 1) the form of language (phonology, morphology, and syntax); 2) the content of a language (semantics); 3) the function of language. (ASHA, 1982)
ROLES AND RESPONSIBILITIES
In considering the roles and responsibilities of the speech pathologist in education, five general areas will be discussed. These will include:
Assessing, describing, and documenting communication behaviors
Evaluating various modes of communication
Developing communication to the fullest extent possible
Developing and evaluating intervention procedures
Providing client advocacy and instructing other professionals
First of all, the speech and language pathologist is responsible for assessing, describing, and documenting the communicative behaviors and needs of each client and then interpreting and integrating these communicative needs with educational and vocational programming. Assessment of speech and language functioning generally involves the following:
a review of developmental, educational, and medical history;
an oral peripheral examination to determine any physical abnormalities that may affect speech;
assessment of articulation, phonation, resonation, respiration;
assessment of prosody and fluency
language comprehension assessment using various standardized as well as informal tests; and,
expressive language assessment using various standardized tests and informal observation generally including a language sample.
After the assessment procedure, children who evidence specific difficulties with auditory language processing, nonfluencies, expressive language delays, articulation errors, etc. should be discussed with those who are in contact with the individual. A clear understanding of the deficit areas and course of treatment should be outlined. Furthermore, it is important to discuss the implications the specific deficits may have on classroom and/or social communications as well as a brief prognosis for improvement.
Second, the speech and language pathologist is responsible for evaluating various modes of communication in light of the individual's abilities and disabilities. This evaluation needs to take into consideration the person's communicative environment in order to develop the most effective means of communication possible. If speech is so severely affected that the prognosis for developing speech is guarded (or extremely remote), it may be necessary to determine what type of augmentative communication system is feasible until such time as speech is a viable method of communication. Gestures, signs, communication boards, electronic devices, etc. may be an effective way to augment
whatever speech may be present.
Third, the speech and language pathologist is responsible for developing speech and vocal communication to the fullest extent possible. In this regard communicative need priorities must be established with the appropriate amount of emphasis on the development of language rather than primarily an emphasis on speech has to be weighed. In the instance of severely physically handicapped children whose speech is nonexistent or virtually impossible to understand it may prove more efficacious and realistic to focus therapeutic efforts on the development of functional language skills rather than speech production per se. Many studies have shown that development of a workable and effective communication system often promotes the acquisition of speech and greatly aids the listener's perception of the communication attempt.
Fourth, the speech and language pathologist is responsible for developing intervention procedures and evaluating their effectiveness in producing or modifying communication. The child's environment as well as the child's abilities have to be taken into consideration. For example, working with the child on the use of a communication board that is made up of written words when he is primarily involved in a classroom of nonreaders is useless to that particular child in that particular environment.
Finally, the speech and language pathologist is responsible for incorporating "significant others" into the intervention plan. This may include family, teachers, or other professionals closely aligned with the child. Integrating the communicative skills/needs of the individual in the home, classroom, and
vocational setting is another responsibility of the speech and language pathologist and requires careful consideration of these various settings to determine the most practical and efficient way of implementing speech and language goals or ideas into these various environments.
DISORDER CATEGORIES - CLINICAL IMPLICATIONS
Having discussed the speech pathologist's roles and responsibilities in education in fairly general terms, it is important to look at the practical applications of these roles and responsibilities in relation to specific disability areas. Each disability area will be briefly discussed in regard to specific
difficulties that may arise at the pre-elementary, elementary, secondary, and/or post-secondary levels.
Cerebral palsy is a term for a group of neurological disorders with etiology in the central nervous system, particularly at the motor control centers. It may result in a range of disabilities including abnormal muscle tone, discoordination or abnormal positioning. Supplemental involvement mey occur in intellectual, perceptual, auditory, speech/language or emotional functioning. (Nicolosi, 1978) Depending upon the severity of the motor involvement, especially oral motor, the child will generally manifest different types of speech and/or language deficits. For instance, the child may be dysarthric. That is, he/she may display impairments of speaking that involve respiration, articulation, phonation, resonation, and/or prosody or a combination of one or more of these. There are several different kinds of dysarthria depending upon the manifestations of motor speech. If speech is mild to moderately affected, then teaching compensatory techniques are generally effective. This involves
such things as over-articulating or slowing down the rate of speaking. If speech is moderately/severely affected, consideration of an augmentative communication system must be entertained. The cerebral palsied the child may have no discernible language comprehension problems. It may be difficult to determine language capabilities if speech is severely affected or if motor impairments prohibit consistent responses to language comprehension testing. It is generally noted that children with cerebral palsy are at risk for learning disabilities based on the very nature of their impairment.
At the pre-elementary level (0 to 3 and 3 to 5 year-old-programs) the speech and language pathologist does the assessment and makes recommendations and referrals as deemed necessary. Goals and objectives are established and intervention may involve direct therapy as well as indirect training of parents and allied professionals. As noted previously, it is important to provide information to those who will be working with the child and to involve them in the speech/language goals in order to maximize progress and carryover. Various methods can be used to incorporate speech and language goals into everyday routines or classroom situations. (Appendix C) Progress reports are filed at the end of the year so that recommendations for future services can be made and speech therapy can be provided on a continuing basis as needed.
At the elementary level, the speech pathologist continues to monitor speech and language development and adjusts goals and objectives accordingly. If a child is using a communication board, it will need to be periodically updated. Since many other disciplines may also be involved, it is important to keep in touch with them not only to let them know what the speech and language pathologist goals are but to incorporate other discipline's goals (such as positioning or fine motor activities) into the speech/language therapy setting. Some school systems utilize the speech/language pathologist more in the classroom in a team-teaching atmosphere while others still rely on the traditional approach of individual therapy in a room apart from the classroom. Some individual teaching may be necessary in order to provide the drill and modify responses as necessary when a skill is first being learned. Carryover into the classroom and monitoring of progress is important as the child has gained more control over a specified skill. Conversely, vocabulary words, concepts, and activities that are being stressed in the classroom can be utilized in the therapy situation as a basis for speech/language goals.
At the secondary level, the child with cerebral palsy often manifests difficulties communicating with peers. If speech is severely affected and an electronic system is in use, the realization that they will never be like the other young people becomes more apparent. Maximizing communication abilities
and modifying communication attempts to be more communicatively competent is often the goal at this level.
At a post-secondary level, the person with cerebral palsy may need to learn language that is more socially appropriate in the different environments in which they find themselves. It is important to remember that these individuals may not have the same kind or "wealth of experiences" that the non-physically handicapped person has. They may need additional help in "reading" the subtle messages that others communicate, including body language. It is important to be aware that at this level communication difficulties continue to manifest themselves as new situations occur.
The next disability category involves the individual with muscular dystrophy also referred to as MD. This disease is marked by weakness of muscles that progresses over time. It is unlikely that these children will survive their teens. Studies have shown that early verbal disability is a characteristic of MD, especially Duchenne's MD. It is a feeling that this is a result of the direct physical influence of the disease upon central nervous system functioning. (Sparks, 1984) Thus, the speech/language pathologist can expect very early verbal impairment which may seem to be more severe than would be expected, given the degree of physical impairment. Goals for speech and language improvement have to be modified as the disease progresses. The main goal of therapy throughout the child's lifespan is to develop and maintain communicative skills which enhance quality of life. For example, a 13-year-old was seen because of gradual decrease in speaking volume. The child could not be heard
in the classroom and listeners had to continually ask, "What did you say?" The individual began to withdraw from speaking situations entirely and became a passive member of the class. He was fitted with a voice amplifier, making his speech more audible. However, this did not result in an immediate improvement of skills. The child had to see that this was accepted by his peers and the peers had to realize that this was an adaptation that would eventually benefit the child.
Another disability category is spina bifida or meningomyelocele. There is a high probability of learning disabilities in those children with low lesions and no hydrocephalus (fluid on the brain). Those children who also have hydrocephalus often have non-verbal intelligence which develops less fully than verbal intelligence. This is because hydrocephalus thins and distends the brain. A distinctive type of language known as the "cocktail party" syndrome appears to be specific to some children with hydrocephalus. These children are often very verbal and have a good memory for social routines as well as adequate articulation. However, most often the conversation is irrelevant and inappropriate. These children find difficulty in using language creatively and will often do poorly on standardized language tests. There is the possibility that "cocktail party" syndrome persists because it is reinforced by the parent and the verbosity of the children is a source of delight and comfort to the parent who may believe that the intellect is unimpaired. (Sparks, 1984) The responsibility of the speech pathologist involves periodic assessment of speech and language functioning to discern any problems at the earliest possible stage. There are no specific manifestations at each grade level and monitoring of communicative competence may be similar to that noted in the next case study.
The last disability category involves the learning disabled child. One known certainty is that early language disorders (preschool) are related to later learning disabilities. Language problems in preschool and school-aged children take a number of forms. Problems reflecting the interactions among language form, content, and use occur in varying degrees and manifest themselves in
comprehension and/or production. These problems change over time and across learning tasks. Researchers who have initiated follow-up studies of children with language disorders early in life suggest that, even after intervention, language disorders persist through the school years and adulthood.
On the preschool level, these children are seen as having delays in the acquisition of speech and language milestones, difficulty attending (sometimes with accompanying hyperactivity), difficulty following directions, and difficulty with the production of language. Intervention usually produces results and often brings the child up to what can be considered "normal" speech and language functioning.
On the elementary level, language disorders often persist but may be more subtle. These disorders manifest themselves as difficulty with word-retrieval, difficulty with auditory language processing, and difficulty with appropriate language usage. These problems are often described*as an "inability to organize thoughts," "fluctuating ability to follow directions," and "language that does not always fit the topic of conversation." Studies have again shown that interventioh will demonstrate progress but when intervention is discontinued, further skills fail to develop or regression is seen. Language problems may also be evident in reading, spelling, and later writing.
On the secondary level, language disorders continue to be evident and are noted in difficulty in dealing with more abstract language, including ambiguities and "underlying" meanings of conversation. Learning disabled children often have difficulty with social interactions because their language is inappropriate in various settings. They miss the subtle meanings and nuances of teenage repartee and are frequently shunned as "weird." Therapy for this population frequently involves role playing and "practicing" appropriate social interchanges in various settings.
On the post-secondary level these same problems persist. However, by now the individual may be more aware of ways to modify the environment or situation to fit his/her specific disability.
In viewing the roles and responsibilities of the speech and language pathologist relative to various disabilities, it can clearly be seen that the scope and degree of speech and language deficits dictate the amount of involvement needed. Present day caseloads of relatively complex cases often leave little time for the interdisciplinary contact necessary for ensuring maximum carryover of a child's "newly-learned" skills. Programs that are structured to meet rigidly defined professional boundaries cannot efficiently (or effectively) provide the services that constitute a total, coherent, integrated approach. Lack of communication among professionals inherent in many autonomously run programs generally leads to misunderstanding and hard feelings, sometimes to the detriment of the child being served. Although there is no "easy" solution, any steps that one can take to maximize understanding of the roles and responsibilities of the other disciplines and to utilize their expertise in a coordinated fashion can ultimately benefit everyone.
REFERENCES
ASHA Membership and Certification Handbook, American Speech-Language-Hearing Association: Maryland, 1984.
"Changes in the Requirements for the Certificate of Clinical Competence," ASHA, Vol. 26(3), March 1984, p. 41.
"Code of Ethics of the American Speech-Language-Hearing Association," ASHA, Vol. 28(4), April 1986, pp. 55-56.
"Communication Disorders and Variations," ASHA, Vol. 11, November 1982, pp. 949-950.
Desk Reference, American Speech-Language-Hearing Association: Maryland, 1985.
Nicolosi, L, Harryman, E., and Kresbeck, J., Terminology of Communication Disorders, Williams and Williams Co.: Baltimore, 1978.
"Requirements for the Award for Continuing Education," ASHA, Vol. 26(5), May 1984, p. 51.
"Serving the Communicatively Handicapped Mentally Retarded Individual," ASHA, Vol 288, August 1982, pp. 547-553.
Sparks, S., Birth Defects and Speech-Language Disorders, College-Hill Press: Calif., 1984., pp. 47-48.
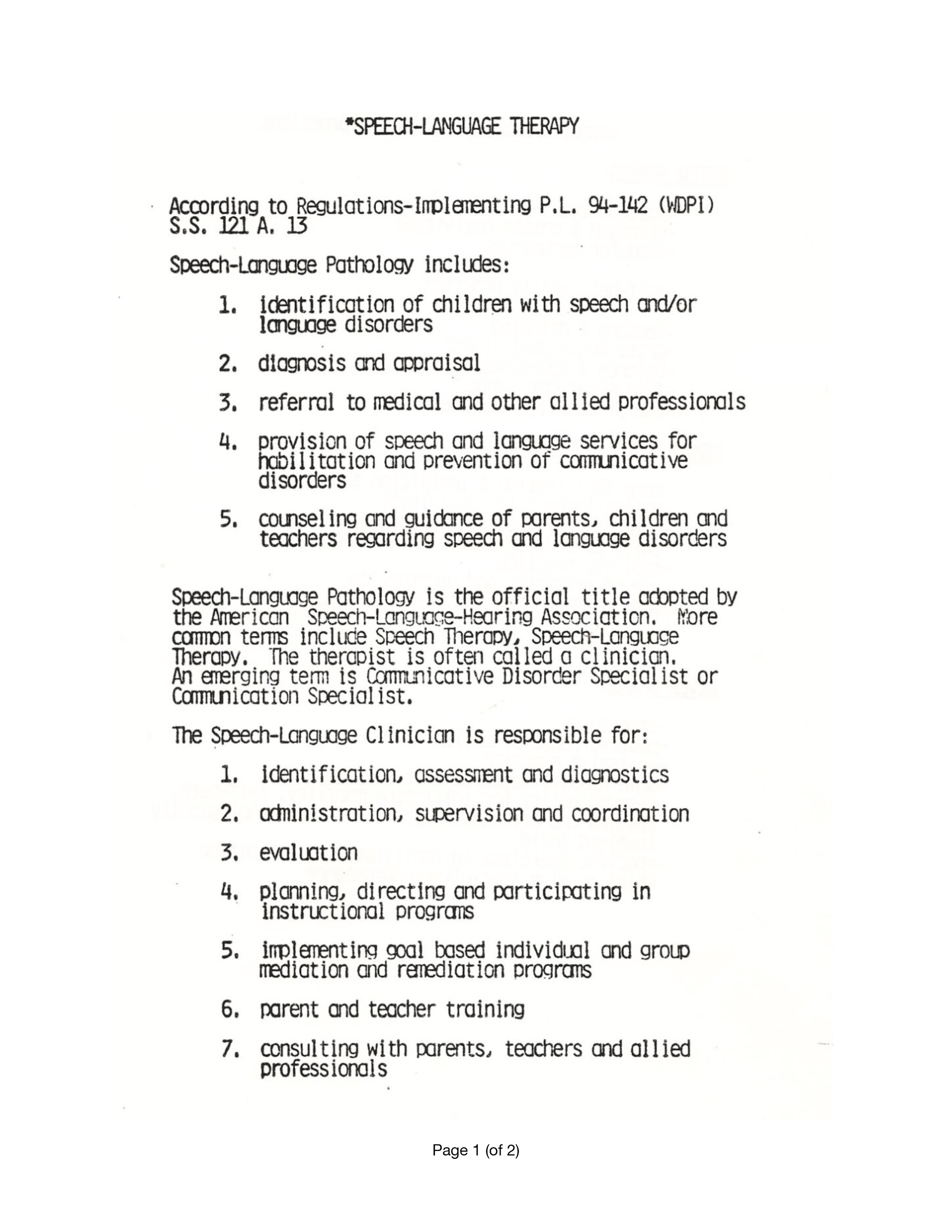
Franks, David J. & Franks, Catherine A., 1981, Speech-Language Therapy.
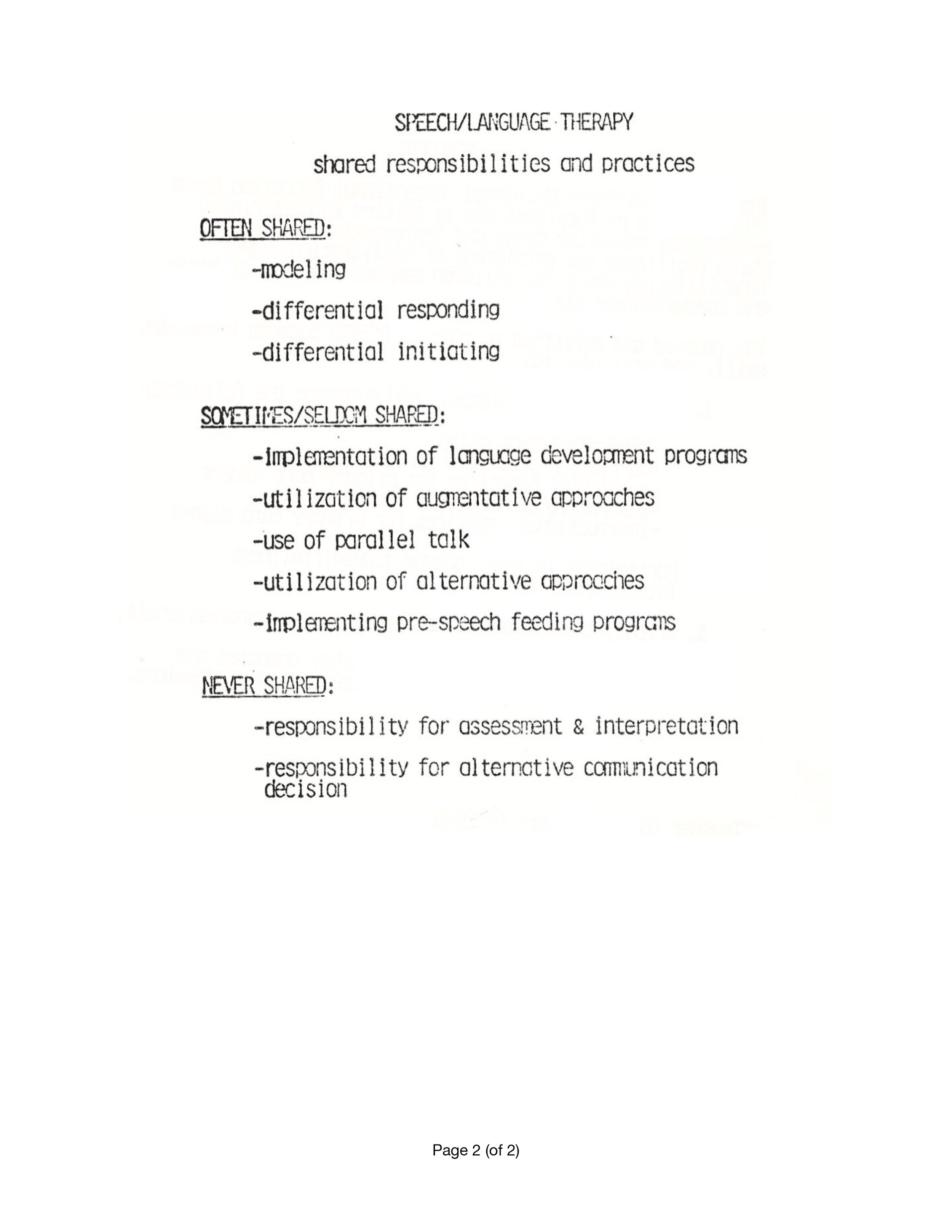
Franks, David J. & Franks, Catherine A., 1981, Trans-disciplinary Practices in Speech-Language Therapy.
Back to the top | Next: Physical Therapy in ECSE >